
By Stephen Bunting, Specialist MSK Physiotherapist (UK)
This article is about Cubital Tunnel Syndrome. Its main aim to is to provide information and advice about the condition with an emphasis on self-help. The information is also provided in video format below.
If you haven't been diagnosed with cubital tunnel syndrome but think you might have the condition then it's best to get checked out first as there are some other conditions that can cause similar symptoms.
The article addresses the condition by answering the 3 most common questions that people ask after they have been diagnosed.
Cubital Tunnel Syndrome is a type of compression neuropathy, meaning it's a problem involving excessive pressure on a nerve. The nerve involved in the condition is called the ulnar nerve which is one of the 3 nerves that supply the hand with sensation and muscle power.
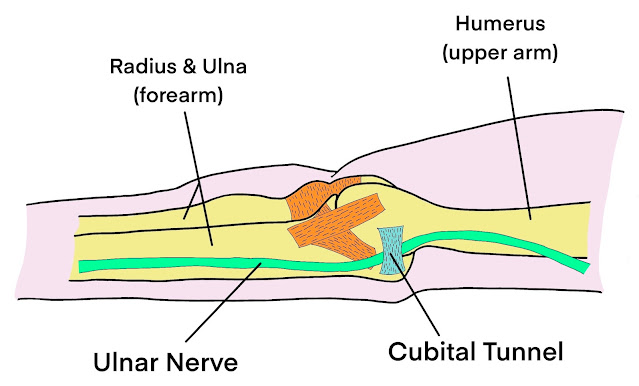
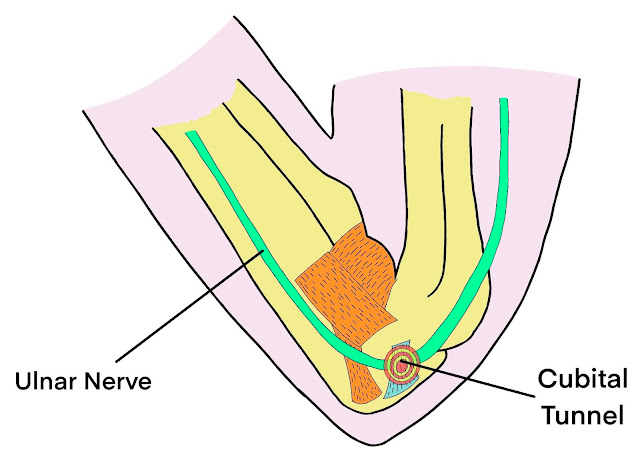
The ulnar nerve travels along the inside of the upper arm, the inside of the elbow and then into the little finger side of the wrist and hand. Nerves are vulnerable to compression when they travel through narrow spaces and the ulnar nerve is vulnerable as it travels through a tunnel on the inside of the elbow, called the cubital tunnel.
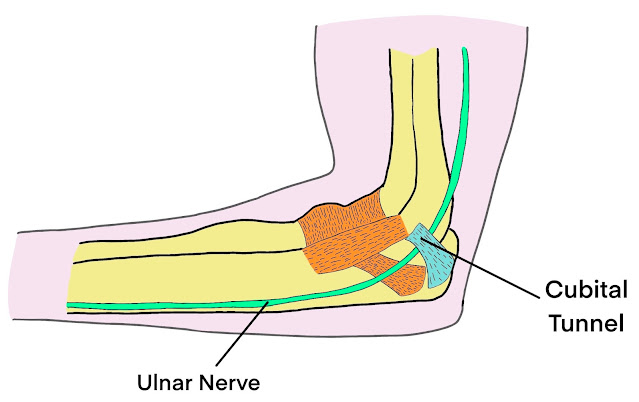 |
| The Course of the Ulnar Nerve at the Elbow |
 |
| The 'Funny Bone' |
The ulnar nerve supplies sensation to the little finger and just half of the ring finger and so the symptoms of cubital tunnel syndrome are usually an uncomfortable tingling sensation in this area. We call this area the ulnar nerve sensory territory.
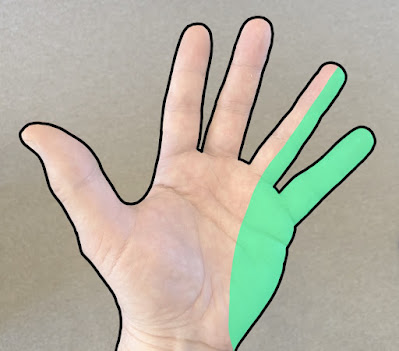 |
| Ulnar Nerve Sensory Territory |
The other common compression neuropathy that affects the other fingers is carpal tunnel syndrome which involves a different nerve called the median nerve. If your symptoms are in the median nerve territory then you're more likely to have carpal tunnel syndrome rather than cubital tunnel syndrome. I've done another article all about carpal tunnel syndrome which you can find here.
 |
| Median Nerve Sensory Territory |
Like most MSK conditions, the symptoms of cubital tunnel syndrome can vary in intensity from mild to severe. Mild symptoms are usually an intermittent tingling sensation in the ulnar nerve territory and people tend to feel it mainly in the little finger.
The symptoms are often worse at night and first thing in the morning but can also occur during the day depending on elbow position and activity. And the reason for this is that the cubital tunnel varies in size according to elbow position. When the elbow is straight the ligament that forms the roof of the cubital tunnel is lax and the tunnel is therefore at its widest position.
With increasing elbow bend, the ligament tightens and at full bend the cubital tunnel is at its narrowest and therefore the ulnar nerve can become compressed in this position.
The main muscles supplied by the ulnar nerve are the small muscles between the fingers and the muscle between the thumb and index finger. A visible wasting of these muscles is a sign of severe cubital tunnel syndrome.
 |
| Muscle Wastage due to Ulnar Nerve Compression |
 |
| Wartenburgs Sign |
It's also worth mentioning that the ulnar nerve can also be compressed at other areas along its course and the next most common area is in the wrist in an area called Guyons canal. Guyons Canal Syndrome is a different condition but the symptoms are very similar to cubital tunnel syndrome, it's just that the ulnar nerve is compressed at the wrist rather than the elbow and it's most commonly seen in cyclists due to prolonged pressure on the nerve from the handlebars pressing on that part of the wrist. I have also seen it in office workers due to excessive pressure through the wrist while typing or using a mouse. A keyboard wrist support, or an ergonomic keyboard and an ergonomic mouse can be helpful.
2) Why have I got it ?

Sleeping with your arms curled up is probably the most common cause and is why the symptoms are often worse at night and first thing in the morning.
Other activities involving prolonged elbow flexion are :-
i) Working with your hands close to your face such as crafting or needlework or perhaps operating machinery.
ii) Some sports, particular those that involve throwing such as baseball, javelin or darts.
iii) Leaning through your elbow for long periods, perhaps while sat at a desk, can also cause the condition.
 |
| Leaning Through the Elbows |
Certain medical conditions can also effect nerve function and therefore make it more likely that someone might develop nerve conditions like cubital tunnel syndrome.
Diabetes, thyroid disease, long term smoking and alcoholism, as well as some vitamin & mineral deficiencies are among a number of conditions that can affect nerve function and make them more vulnerable to developing neuropathies like cubital tunnel syndrome. A simple blood test can often screen out these conditions so its worth getting checked out if your symptoms don't settle down.
Diagnosis
 |
 |
| The Tinel's Test |
One of the best tests is to check the sensation of your fingers with a tissue at a time when you have the tingling or numbness feeling. If you feel the sensation is reduced in the little finger when compared to the index finger or thumb, and particularly if the sensation is reduced in the little finger side of the ring finger compared to the other side, well thats good evidence for cubital tunnel syndrome.
Another test thats sometimes used and you can do this yourself, is the Tinel's test. Tapping the area where the nerve lives on the inner elbow may cause that familiar shooting pain or tingling feeling.
Test the other side for comparison though as a normal nerve can sometimes feel uncomfortable during this test and its only considered positive if there is a significant difference between your 2 elbows.
If the diagnosis isn't obvious or your clinician thinks there might be other causes of your symptoms then you might be sent for something called Nerve Conduction Tests. This can assess the function of the nerves in your arm in more detail and help to provide the clinician with further information from which to help make the diagnosis, or to determine the severity of the condition which can help when planning treatment.
 |
| Nerve Conduction Tests |
3) Why can I do about it ?
For people with just the tingling symptoms but no muscle weakness or muscle wastage then the prognosis for recovery is very good. Indeed the majority of people will get fully better within about 9 months from the first onset if symptoms. This is because nerve recovery occurs at about 1mm per day from the site of compression and if you do the maths for the ulnar nerve, that works out at about 9 months for most people.
To help encourage the healing process the most helpful thing you can do before anything else is to try and identify and then reduce or stop any activities where you might be bending your elbow excessively for long periods.
 |
| Amazon link to a suitable splint |
However, for a splint to work, it doesn't need to keep your elbow fully straight it just needs to stop you from bending it all the way up.

 |
| An 'Alternative' option for restricting Elbow Flexion |
Another self help treatment that might be worth trying is Anti-Inflammatory Gel rubbed into the cubital tunnel region 3-4 times daily over a few weeks. Because the nerve is close to the skin surface, the gel can easily reach it and help to settle any inflammation. Please talk to a pharmacist or a prescribing clinician first though as not everyone can use anti-inflammatories.
And that may be all the treatment you need. Like I said, Cubital tunnel syndrome will tend to slowly get better by itself over about 9 months once you've stopped or reduced the elbow bending activity that is aggravating the nerve.
There is also some evidence to support the use of nerve gliding exercises to help stimulate nerve recovery. Simple movements involving elbow bending and straightening will slide the nerve through the cubital tunnel and potentially help with the healing process. Ive made a video showing 3 good exercises for cubital tunnel syndrome which you can see below.
If all of that doesn't help then you might need to see a specialist clinician about further treatment. Some clinicians may suggest a cortisone injection into the cubital tunnel to help reduce inflammation around the nerve but the evidence for this isn't great and it’s therefore becoming less commonly used over recent years.
Another procedure called nerve hydro-dissection is starting to become more popular. This involves injecting sterile water or local anaesthetic under ultrasound image guidance, carefully around the nerve to try and separate it from surrounding scar tissue that can build up over time. Early results are promising for mild to moderate cases of cubital tunnel syndrome but it's a skilled procedure that only tends to be available at specialist centres.
Finally, If you have a stubborn case of cubital tunnel syndrome that isn't showing any signs of improvement after 6-9 months then you may need to talk to an upper limb surgeon about the option of surgery to decompress the nerve. Also, if you have any of the muscle weakness symptoms or visible hand muscle wastage described earlier then you probably have more severe ulnar nerve compression which is less likely to get better by itself and will usually need surgical treatment.
A few different procedures are used but the most common one is the ulnar nerve anterior transposition where the surgeon frees the nerve from the cubital tunnel and then moves it further forward to a position where it doesn't become squashed when the elbow is bent.
I hope the article has been helpful in teaching you ways of treating cubital tunnel syndrome yourself and we've discussed some of the other treatment options available if symptoms don't improve as hoped.
__________________________________________________________________________
This article provides general information related to various medical conditions and their treatment. It is intended for informational purposes only. It is not a substitute for professional advice, diagnosis or treatment provided by a doctor or other qualified health care professional. The information provided does not constitute personal advice or guarantee of outcome and should not be used to diagnose yourself or others. You should never ignore advice provided by a health care professional because of something you have seen or read on this website. You should always consult a doctor or other qualified health care professional for personal medical advice.